aortic dissection in pregnancy
- related: OBGYN
- tags: #obgyn
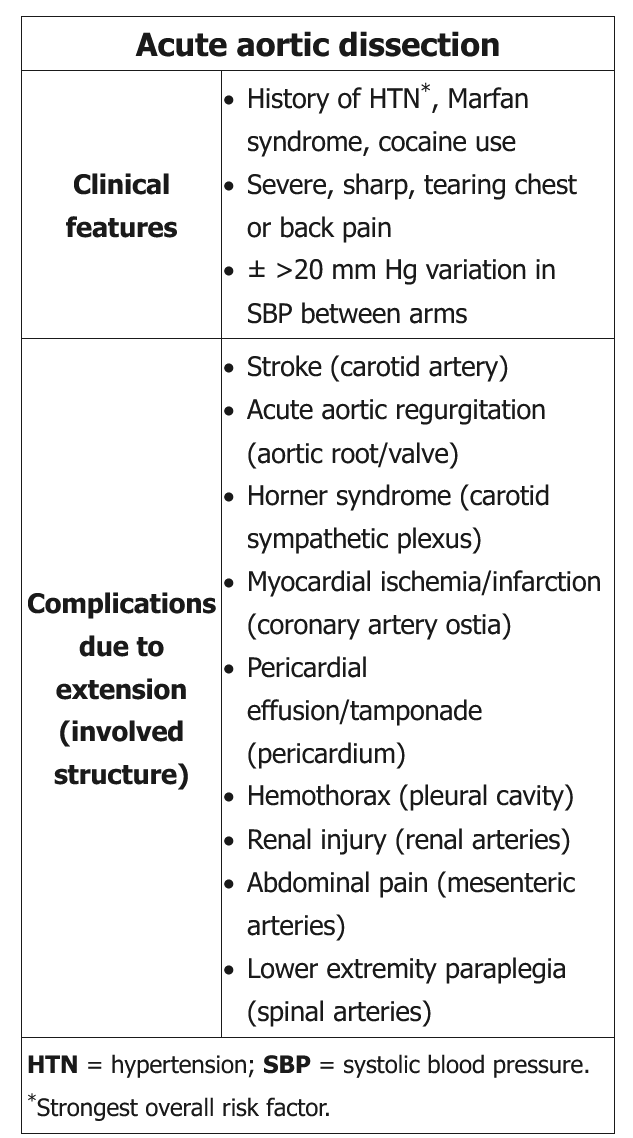
This pregnant patient with hypertension, chest pain, and Horner syndrome likely has a peripartum acute aortic dissection. Spontaneous dissection of the aorta and coronary arteries can occur in pregnancy, most commonly in the third trimester, due to the hyperdynamic state and hormonal effect on vasculature. Horner symptoms, (anisocoria, ptosis) are due to the dissection extending into the internal carotid artery and externally compressing the left superior cervical sympathetic ganglion. Patients may also present with vocal cord paralysis due to compression of the left recurrent laryngeal nerve. Pulse deficits are classic, but they are seen in <30% of patients and are less common in women.
Multiple imaging modalities may be used for diagnosis of aortic dissection, with the choice of study dependent on the patient and imaging availability.
-
CT angiography is most commonly used due to its widespread availability in emergency departments and rapidity; however, if possible, CT scans should be avoided during pregnancy due to radiation exposure to the fetus.
-
Transesophageal echocardiography can be performed quickly by a cardiologist in the emergency department and avoids radiation exposure. Transthoracic echocardiography is a less sensitive and specific alternate because it may fail to adequately assess large portions of the aorta, particularly in pregnant women.
-
MR angiography is generally a slower modality but avoids radiation and does not require iodinated contrast.
(Choice A) Cardiac catheterization is usually indicated for acute coronary syndrome (ACS), which may present as acute-onset chest pain. However, this patient's age, sex, and nonspecific ECG findings make ACS very unlikely.
(Choice B) Magnesium is used for seizure prevention in preeclampsia, which presents with hypertension and may cause edema, visual disturbances, abdominal pain, and headaches. However, the presence of Horner syndrome (ptosis, anisocoria) and the absences of proteinuria and, in particular, of hyperreflexia make aortic dissection more likely than preeclampsia.
(Choice C) Nitroprusside use is contraindicated in pregnancy due to possible risk of fetal cyanide poisoning. In patients with suspected aortic dissection, beta blockers are first-line agents for blood pressure control. Nitroprusside can be added if goal systolic blood pressure (eg, 100-120 mm Hg) is not achieved; however, its use alone can cause reflex sympathetic stimulation, leading to increased left ventricular contractility and aortic wall shear stress with potential risk of propagation of aortic dissection.
(Choice D) MRI of the head is used to evaluate for an acute stroke, which could cause Horner syndrome but would not be expected to cause chest or abdominal pain.